Eurobio Oncology
Prolaris®: Clinicians
Enhance your Patient’s Prostate Cancer Management
Prolaris provides the precision needed to tailor treatment strategies in localized prostate cancer1-5
Prostate cancer treatment decisions can be hard
-
Prostate cancer ranges from indolent tumors to aggressive disease requiring urgent treatment. Determining whether your prostate cancer patients are safe for active surveillance or would benefit from single- or multi-modal treatment can be challenging.
- Standard clinicopathological parameters remain fundamental to risk stratification but are not always sufficient for definitive decision-making. Interobserver variability in histopathological grading - particularly in Gleason scoring - can contribute to uncertainty in risk classification and therapeutic planning.6-9

Comprehensive Risk Assessment for Localized Prostate Cancer
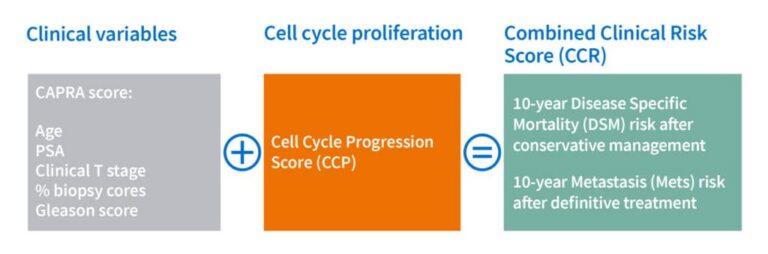
The Prolaris test quantifies the expression of cell cycle progression (CCP) genes in prostate tumor tissue. The CCP score reflects the biological aggressiveness of the individual tumor – specifically its proliferative potential. This molecular CCP score is combined with established clinical-pathological factors (CAPRA score) to deliver a Combined Clinical Risk Score (CCR).
This integrated score provides an individualized 10‑year estimate of Disease‑Specific Mortality (DSM) for patients managed conservatively as well as an individual 10-year estimate of Risk of Metastasis (Mets) after definitive local therapy (surgery or radiation).1-5
It adds significant prognostic power to traditional prostate cancer risk assessment methods, providing you with the confidence to develop the right treatment plan.2
Providing Answers to Critical Treatment Questions
Prolaris helps identify which men with localized prostate cancer are appropriate for active surveillance and which require active treatment, as well as which patients may need single-modal therapy versus multi-modal treatment.1-5
Using two separate clinically validated cut-offs, Prolaris stratifies patients as follows:
Active surveillance vs. single-modal treatment
Prolaris provides a personalized estimate of 10-year disease-specific mortality under conservative management, helping you and your patients make confident decisions between active surveillance and single-modal treatment.1-3
Single-modal vs. multi-modal treatment
Prolaris provides a personalized estimate of 10-year metastasis risk following single-modal treatment, helping you and your patients make confident decisions about adding further therapies when appropriate.4,5
Identify active surveillance (AS) candidates at biopsy
Prolaris enables the identification of men with low progression risk who may be eligible for active surveillance, while separating them from those who may benefit from definitive single‑modal intervention such as surgery or radiation.1-3
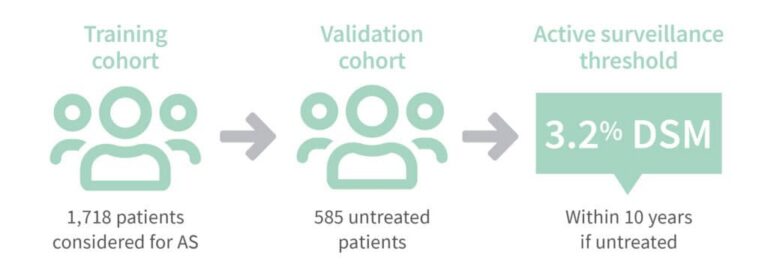
The test was developed and validated specifically in untreated men, making its use in AS discussions particularly relevant and precisefor your daily clinical practice.1
The validated cut‑off for AS is 3.2% 10‑year Disease‑Specific Mortality (DSM) risk in untreated patients. In the Prolaris validation study, there were no deaths from prostate cancer below this threshold, demonstrating the assay’s strong predictive value.¹
This ensures confident identification of patients who can avoid immediate intervention without compromising outcomes.
Identify patients who require definitive therapy and the appropriate intensity of intervention
A higher Prolaris score threshold identifies men at elevated risk who may benefit from multi-modal treatment approaches, such as combining definitive local therapy (surgery or radiation) with androgen deprivation therapy (ADT) to improve long-term outcomes.
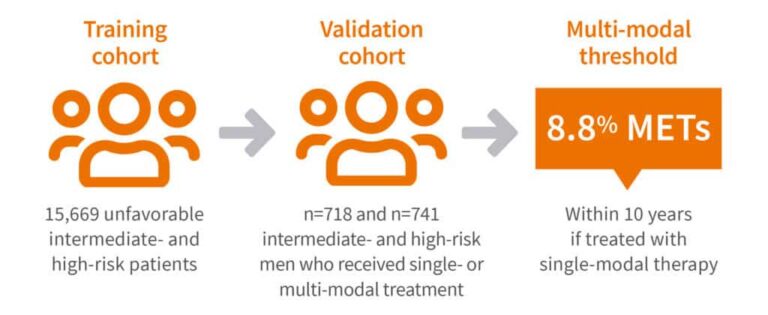
This multi-modal threshold was developed and double-validated in treated men to predict the 10-year risk of metastasis and to determine which patients may not benefit from multi-modal therapy. The cut-off is defined as an 8.8% metastasis risk (Mets) within 10 years in patients treated with single-modal therapy (surgery or radiation).4,5
Clinical data show that patients below this threshold derive little to no benefit from combined multi-modal therapy, while those above the threshold experience a significant benefit from the addition of ADT.10
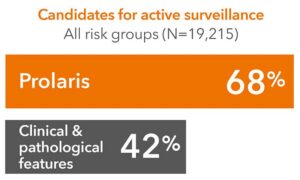
In a large clinical utility cohort of over 19,000 men across all risk groups, Prolaris identified 68.8% of patients as eligible for active surveillance – compared to only 42.6% when using clinicopathological features alone. The 10-year predicted prostate cancer specific mortality was nearly identical between the two groups (1.9% vs. 2.0%), demonstrating, that Prolaris test–informed decision‑making enables more men to pursue active surveillance instead of immediate Intervention.1
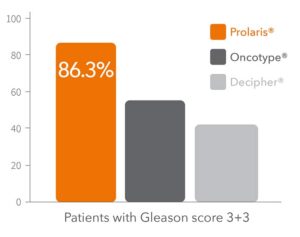
In an independent study, Prolaris outperformed other genomic tests in identifying men suitable for active surveillance. Among low-risk (Gleason 3+3) patients, 86% were below the Prolaris AS threshold.11 Prolaris is the only biomarker with an AS threshold validated in conservatively managed patients, allowing clinicians to recommend active surveillance with greater confidence.1
Eligibility for Prolaris® Testing
Prolaris provides essential insights to guide treatment decisions for men with localized prostate cancer who meet the following criteria:
- Localized prostatic adenocarcinoma (after diagnosis or under active surveillance)
- Tumor size pT1 to pT3a
- PSA levels ≤100 ng/ml at diagnosis
- All risk categories
- Adequate tumor tissue available from biopsy
Prolaris can be applied to any risk group but is recommended by international and national guidelines when the result is expected to influence or clarify treatment planning – such as when clinicopathological findings alone leave uncertainty.12-17 The test can be performed on FFPE tumor tissue from diagnostic biopsy.

Fast, Clear, and Actionable:
Prolaris® Result Report
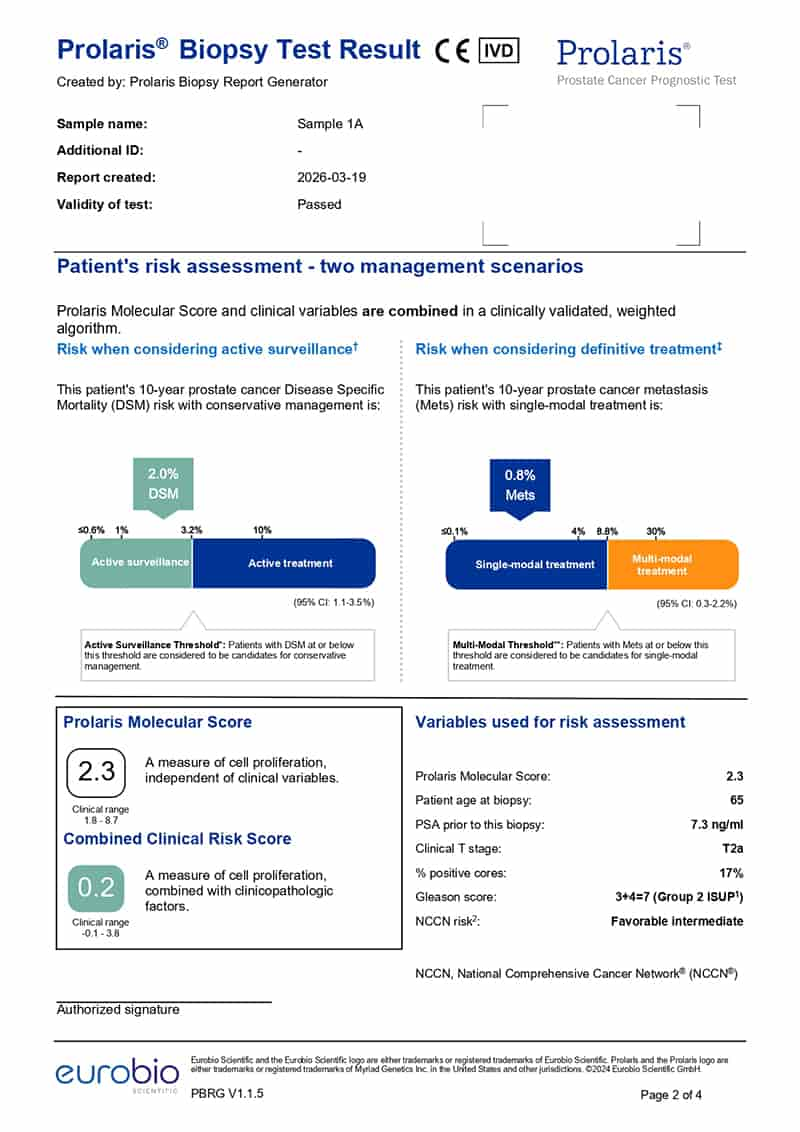
The Prolaris report combines the Cell Cycle Progression (CCP) score with standard clinical and pathological factors to generate the Clinical Cell Cycle Risk (CCR) score – a validated predictor of prostate cancer progression.
It provides actionable insights to guide treatment decisions for men with localized prostate cancer:
- Whether active surveillance is appropriate based on 10-year Disease-Specific Mortality risk with conservative management
- Whether additional therapy may be warranted based on 10-year metastasis risk with single-modal treatment
Results are presented in a clear, intuitive, user‑friendly format, including visual thresholds and patient-oriented summaries, helping clinicians communicate risk effectively and support shared decision-making.
By integrating genomic data with clinical variables, the CCR score enables personalized treatment planning and confidence in selecting the most appropriate management pathway.
How Prolaris® Testing Works
- Find your local lab
Contact your local pathology laboratory offering Prolaris to benefit from a fast turnaround time. Find a list of participating laboratories in the test access and ordering section.
- Send your sample
Tumor samples should be from a diagnostic biopsy performed prior to any treatment. The lab will provide further information on preparing and sending the sample.
- Fast results
Once the lab has received the sample, results can be returned within a week, allowing you and your patient to make important treatment decisions without delay.

Prolaris is a CE‑certified in vitro diagnostic (IVD), licensed from Myriad Genetics. The test measures the expression of 10 cell cycle progression (CCP) genes and 6 housekeeping reference genes to generate the molecular risk score. While the European kit panel contains fewer genes than the original US‑based Myriad test, it has been validated to provide the same accuracy for localized performance outside of the US.18

Prolaris® in Guidelines
International and national guidelines such as ASCO, AUA/ASTRO, EAU, DEGRO, APCCC, and the German S3 guideline cite Prolaris as a potential additional decision-support tool when a clear therapy recommendation cannot be made based on clinicopathologic factors alone.12-17
Precise testing
Prolaris provides precise risk stratification by combining CAPRA with an independent gene expression score based on cell cycle proliferation (CCP).
Tailored results
Prolaris is the only test with thresholds for active surveillance validated in untreated patients and for multimodality treatment decisions based on studies that included patients treated with different therapeutic regimens.1-5
Empowered decisions
Prolaris delivers validated risk stratification across all NCCN risk groups - guiding decisions from active surveillance to multimodal therapy with confidence.
References
Lin DW, et al. Identification of men with low-risk biopsy-confirmed prostate cancer as candidates for active surveillance. Urol. Oncol. 2018
Cuzick J, et al. Prognostic value of a cell cycle progression signature for prostate cancer death in a conservatively managed needle biopsy cohort. Br J Cancer. 2012
Cuzick J, et al. Validation of an RNA cell cycle progression score for predicting death from prostate cancer in a conservatively managedneedle biopsy cohort. Br J Cancer. 2015
Tward JD, et al. Personalizing localized prostate cancer: Validation of a combined clinical cell-cycle risk (CCR) score threshold for prognosticating benefit from multimodality therapy. Clin Genitourin Cancer. 2021
Tward JD, et al. The clinical cell-cycle risk (CCR) score is associated with metastasis after radiation therapy and provides guidance on when to forgo combined androgen deprivation therapy with dose-escalated radiation. Int J Radiat Oncol Biol Phys. 2022
Liss, MA, et al. Prostate Cancer Biomarker Development: National Cancer Institute’s Early Detection Research Network Prostate Cancer Collaborative Group Review. Cancer Epidemiol Biomarkers Prev. 2020
Allsbrook WC, et al. Interobserver reproducibility of Gleason grading of prostatic carcinoma: Urologic pathologists. Hum. Pathol. 2001
Schreiber D et al. Prostate biopsy concordance in a large population-based sample: a Surveillance, Epidemiology and End Results study. J. Clin. Pathol. 2015
Oshikiri T, et al. Prognosis of patients with prostate cancer and middle range PSA levels (20–100 ng/mL): When PSA reaches approximately 70 ng/mL, prognosis may plateau. Int Braz J Urol. 2016
Tward JD, et al. Using the Cell-Cycle Risk Score to Predict the Benefit of Androgen-Deprivation Therapy Added to Radiation Therapy in Patients With Newly Diagnosed Prostate Cancer. JCO Precis Oncol. 2024
Hu J.C. et al. Clinical Utility of Gene Expression Classifiers in Men With Newly Diagnosed Prostate Cancer. JCO Precis Oncol. 2018
Leitlinienprogramm-Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Prostatakarzinom, Langversion 8.1, 2025, AWMF-Registernummer 043-022OL
EAU: EAU Guidelines. Edn. presented at the EAU Annual Congress Madrid 2025. ISBN 978-94-92671-29-5.
APCCC: Management of patients with advanced prostate cancer—metastatic and/or castration-resistant prostate cancer: report of the Advanced Prostate Cancer consensus Conference (APCCC) 2022S. Gillessen et al. / European Journal of Cancer 2023
DEGRO: Combs SE, Belka C, Budach W, et al. Biomarkers in prostate cancer: current status and future directions in radiotherapy—statement from the Prostate Cancer Working Group of the German Society of Radiation Oncology (DEGRO). Strahlentherapie und Onkologie 2025
Eggener S.E.et al. Molecular biomarkers in localized prostate cancer: ASCO guideline. J Clin Oncol 2020
- Eastham J.A. et al. Clinically localized prostate cancer: AUA/ASTRO guideline, part I: introduction, risk assessment, staging, and risk-based management. J Urol. 2022
Kuhl V, et al. Development and validation of a cell cycle progression signature for decentralized testing of men with prostate cancer. Biomark Med. 2022